Tactical First Aid
TCCC and the MARCH algorithm - Learn to save a life

In today’s post we'll be going over the MARCH algorithm.
I didn't plan on writing a post about first aid this early, but recent events have convinced me that this is something everyone should know.
A wise man once said that knowing how to plug holes is just as important as knowing how to make holes.
It was me. I said that.
The MARCH algorithms is an essential part of TCCC – Tactical Combat Casualty Care. While developed for military use, I have seen it successfully adapted in a civilian context on multiple occasions.
It is my firm belief that the MARCH algorithm should be known by everyone who wants to have the ability to help himself or others in case of a casualty event.
First of all, hat is the point of TCCC/MARCH?
TCCC was developed using best practices for medical treatment form the point of injury to evacuation to a medical facility.
Simply put, the goal of applying MARCH is to keep a casualty alive in the field until proper care can be provided.
The success of TCCC has been well documented and it has been used to save countless lives.
Lets get down to the MARCH algorithm. The MARCH acronym stands for:
M – Massive haemorrhage
A – Airway
R – Respiration
C – Circulation
H – Hypothermia/head injury
and it is used to remember the proper order of treatment.
CAVEAT!!: Before starting to apply the MARCH algorithm, you need to be sure the area you are operating in is secure.
In a combat environment, this means the enemy has been neutralized and the casualty has been moved away from the immediate combat zone.
In the case of an active shooter, your main goal should be to neutralize the active shooter before starting to apply first aid.
So, lets break down the algorithm
1. Massive hemorrhage
A.k.a. bleeding, is the primary treatable cause of death from traumatic injury. In fact, over 90% of post 9/11 USA combat deaths were from hemorrhage induced injuries.
Read that again.
When treating bleeding we have two main courses of action.
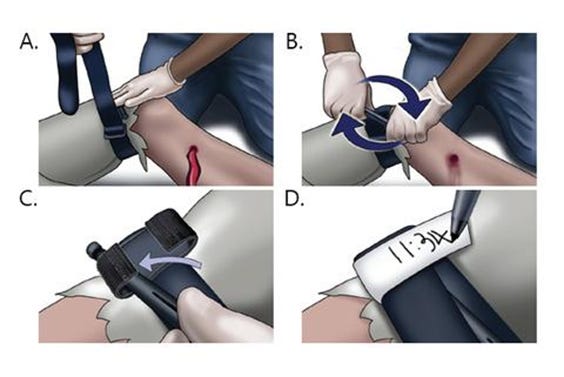
If the source of the bleeding in on a limb, apply a tourniquet (pictured).

Pictured is the CAT-T tourniquet. I won’t claim that it’s the best tourniquet, but its one I’ve trained with and use. It works. That’s good enough for me.
In fact, if I could recommend one thing for you to carry everywhere you go, it’s a TQT. You’ll probably never need it. But if you need it, you *REALLY* need it.
How to apply the tourniquet? I could write an entire thread only on that topic.
Basically, the most common advice is to apply it *high and tight* meaning you slap it on as high on the wounded limb as possible. Then you turn the windless (the stick) as far as it will go. And then some more. It will hurt. But hurting is better than bleading to death.
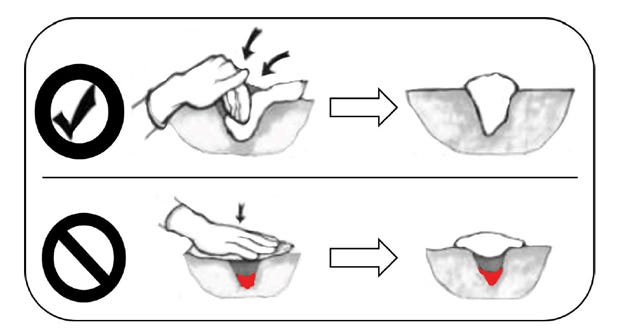
The second way to stop the bleed, when applying a TQT is not an option, is packing the wound. This one is simple.
1. Take gauze
2. Shove gauze into the wound as far as it goes
2. Airway
Check if the casualty’s airway is clear.
Is the casualty yelling? It means the airway is clear.
So does crying, cursing, complaining.
No sound? Check the airway. Best be is to visually check the airway for obstructions and audibly check if the casualty is breathing. If we are not sure, time to insert the NPA.
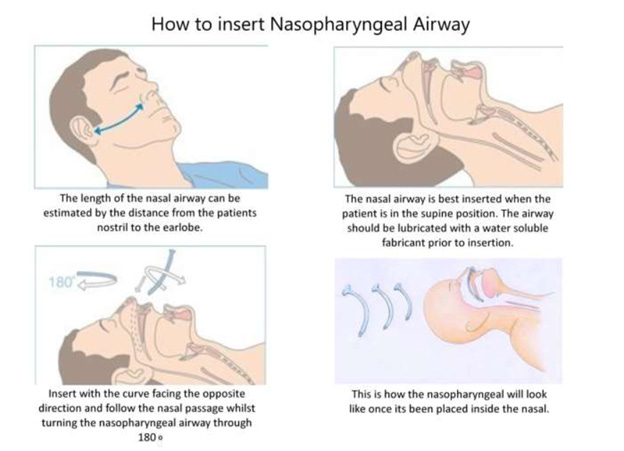
Pro tip – lube that baby up like there’s no tomorrow.
Another thing you can do is a Cricothyroidotomy AKA a Cric. If you are learning about TCCC from this substack, pretend you didn’t read the last sentence and move on.
NOTE: BowTiedFireFighter wrote a very extensive substack post on airway management, go check it out!


3. Respiration
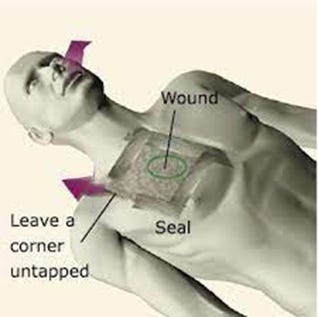
Having a hole in your chest often has the nasty side effect of developing atension pneumothorax (PTX).
Basically, air trapped in the chest cavity begins pushing on the lung tissues and heart causing an inability to breathe and inducing a cardiac arrest.
Fortunately, this is easily preventable. Slap on a chest seal over the entry wound (don’t forget to check for exit wound, those need a chest seal too!!).
Using a needle chest decompression (NCD) is also an option. If you are learning about TCCC from this substack, pretend you didn’t read the last sentence and move on (Déjà vu?).
4. Circulation
At this point, you want to determine if the casualty is falling into shock. Falling into shock is no bueno.
The telltale signs of shock are:
a) Increased pulse (>120/min) or slow pulse (<50/min)
b) Perfusion – cold, clammy skin; blue lips, altered mental state (“I’m gonna apply for BUDS and be a SEAL!”, MF, we’re army)
c) Blood pressure - low blood pressure
5. Hypothermia
Hypotermia means the casualty is very cold. What you want to do is make them warm.
If the casualty has wet clothes, remove them and replace with dry clothes. Wrap casualty in foil blanket. Track temperature.
If possible, provide warm liquids.
Thats is, a very high level overview of the MARCH algorithm. While the advice in this post are actionably, my advise is to get in person training if possible.
As always, I’m open for any questions.
Thank you for reading
Stay safe!
NOTE: THIS IS NOT MEDICAL, LEGAL, LIFE OR RELATIONSHIP ADVICE. SERIOUSLY, CHECK YOUR LOCAL LIABILITY LAWS. GET TRAINING. BE SMART.